
VisionCheck in Pediatric Refractive Screening
Scalable, objective refractive screening for children using only a smartphone
Why Pediatric Refractive Screening Still Needs Better Tools
Uncorrected refractive error remains one of the most common and treatable causes of reduced vision in children worldwide. The burden is not only visual; delayed detection can affect neurovisual development, school performance, and long-term quality of life. In early childhood, missed refractive error can increase the risk of amblyopia during the period when treatment is most effective. This makes timely and scalable screening essential.
Current screening pathways within vision health care rely on tools such as autorefractors, retinoscopy, and photoscreeners. These methods can perform well in clinical environments, but they also introduce practical constraints: dedicated hardware cost, operator training requirements, workflow variability, and limited portability outside specialist settings.
VisionCheck is designed to address this gap as a software-first screening tool. It uses a standard smartphone camera and analyses the refractive signal from the pupil reflex geometry without dedicated optical hardware. The output is screening-oriented: it classifies the subject as myopic, hyperopic, or exhibiting no refractive error signal. A key advantage in paediatrics is objectivity, since measurement does not depend on subjective responses from the child.
A major opportunity for VisionCheck lies in environments where trained eye-care professionals are not readily available. Schools, community health programs, and remote screening initiatives often serve large numbers of children but lack the clinical expertise or specialised equipment needed to reliably detect refractive errors. Since VisionCheck requires no optical training, it enables non-clinical staff, such as school nurses, teachers, or community health workers, to perform preliminary vision screening consistently and objectively. This expands the reach of early detection efforts, helping identify children who need full clinical evaluation.
In this technical write-up, we evaluate VisionCheck in pediatric use through two complementary datasets:
- A prospective clinical experiment in Aarhus Ophthalmology Centre pediatric workflows.
- A retrospective age-stratified analysis from ProApplabelled real-world data.
In parallel, our analysis of the OptikosPrime pupil-iris segmentation model outputs identified a consistent pupil-diameter difference between children and adults in our data. This trend is also aligned with published ophthalmic literature [1] [2]. In practical terms, this supports greater signal in children, making refractive warning signals easier for VisionCheck to detect.
Terminology
- ProApp is OptikosPrime’s data collection app used by opticians to collect labeled data
- Argus is OptikosPrime’s AI-driven refraction tool designed to provide users with a full prescription from just a phone photo
- VisionCheck is OptikosPrime’s phone-based screening tool that is designed to simplify the process of eye health assessment.
Key Findings
- Clinical cohort: 88.9% classification accuracy in pediatric patients (Aarhus feasibility study).
- Retrospective pediatric accuracy: 85.1% on conclusive predictions.
- Physiological signal: children show larger pupil diameters than adults (+0.69 mm median difference).
- Interpretation: larger pupils increase refractive crescent visibility, improving screening signal quality.
The real promise of VisionCheck is its ability to extend high-quality refractive screening beyond traditional clinical walls. In schools, community programs, and regions without trained eye-care personnel, we often see the greatest unmet need. A tool that can deliver objective, repeatable refractive-error screening using only a smartphone has the potential to transform early detection. It enables non-clinical staff to quickly identify at-risk children and refer them for eye exams sooner. This kind of scalable, accessible technology could meaningfully reduce the global burden of uncorrected refractive error.
Tony Pansell, Professor in Optometry, Karolinska Institutet
Clinical Experiment: Aarhus Ophthalmology Centre
As an initial pediatric evaluation, VisionCheck was tested in collaboration with Aarhus Ophthalmology Centre in a cohort of 18 children aged 12 years or younger. The objective of this experiment was to assess whether VisionCheck performs reliably in pediatric subjects — specifically, whether children can complete the capture protocol and whether the system maintains comparable screening accuracy in this age group.
Using the pediatric reference labels available for this cohort, VisionCheck produced 16 correct predictions out of 18 cases, corresponding to 88.9% classification accuracy.
- Total pediatric cases: 18
- Correct predictions: 16
- Overall accuracy: 88.9%
This result is consistent with the expected model behaviour observed in prior validation studies (~90%), suggesting that VisionCheck maintains similar performance when applied to pediatric subjects in a clinical workflow.
The class distribution in this feasibility cohort was imbalanced toward hyperopia:
- Hyperopia: 15 cases
- Myopia: 2 cases
- Emmetropia: 1 case
Confusion matrix (Aarhus pediatric feasibility):
-.png)
Within this cohort, the myopia and emmetropia cases were correctly identified, while the small number of misclassifications occurred within the majority hyperopia class. Both hyperopic misclassifications were associated with low-quality video capture and subject movement during acquisition, which likely degraded the refractive signal and contributed to the incorrect predictions.
An additional operational observation during pediatric capture was stronger flash-induced pupil dilation in younger subjects. Larger pupil apertures can increase the visibility of refractive signals under standard capture conditions [3] [4], which may support robust VisionCheck signal detection in pediatric screening scenarios.
Retrospective Validation: ProApp Pediatric Cohort (<15 years)
To complement the Aarhus feasibility cohort, we performed a retrospective analysis using ProApp measurements that include age metadata. VisionCheck predictions were generated using the same inference pipeline as the screening workflow, allowing evaluation of pediatric performance on a larger real-world dataset.
The analysis was restricted to samples matching the intended screening conditions and quality controls used by the application.
- Only vertical images from ProApp measurements were included
- Cylinder-based filtering was applied during data extraction. Subjects with a cylinder stronger / higher than −5 diopters were excluded
- Extremely short camera-to-subject distances were removed prior to accuracy calculation
- A manually reviewed list of problematic IDs was excluded. 10 subjects where the autorefractor label was considered unreliable were removed from the final evaluation
Because VisionCheck is designed as a screening system, predictions may be either conclusive (myopia, hyperopia, emmetropia) or inconclusive if image quality or capture geometry does not meet the predefined inference criteria. To avoid conflating capture quality with diagnostic performance, classification accuracy was evaluated only on conclusive predictions.
For pediatric subjects (age < 15), the conclusive subset used for accuracy evaluation contained 47 images of eyes. Within this subset, VisionCheck achieved:
- Accuracy (pediatric, conclusive only): 85.1%
- Weighted F1 score: 85.3%
Class distribution within the pediatric conclusive subset was:
- True labels: up=32, down=8, none=7
- Predicted labels: up=29, down=10, none=8
Confusion matrix for the pediatric conclusive subset:

Overall, the retrospective ProApp analysis shows that pediatric captures maintain strong classification accuracy once quality constraints are satisfied.
One hyperopic case (2 eyes) was misclassified as myopic from a low-quality capture. Manual review showed an atypical superior blue-toned crescent; chromatic crescent coloration has been described in photorefraction literature, but its interpretation is setup-dependent, making this sample an uncommon edge-case appearance that is underrepresented in the current training data. [^5]
Pupil Size and Pediatric Signal Geometry
During exploratory review of the data, we observed a pattern suggesting differences in pupil size in pediatric subjects. To quantify this observation, we analysed pupil size using the OptikosPrime pupil–iris segmentation model on the ProApp images corpus.
Pupil Size Analysis
For each image with a valid iris and pupil circles, pupil diameter was estimated in millimetres using the trained pupil and iris segmentation model of OptikosPrime. Only images where both pupil and iris circles were successfully detected were included. All the other data are included in the analysis, including small camera to subject distance and inconclusive data.
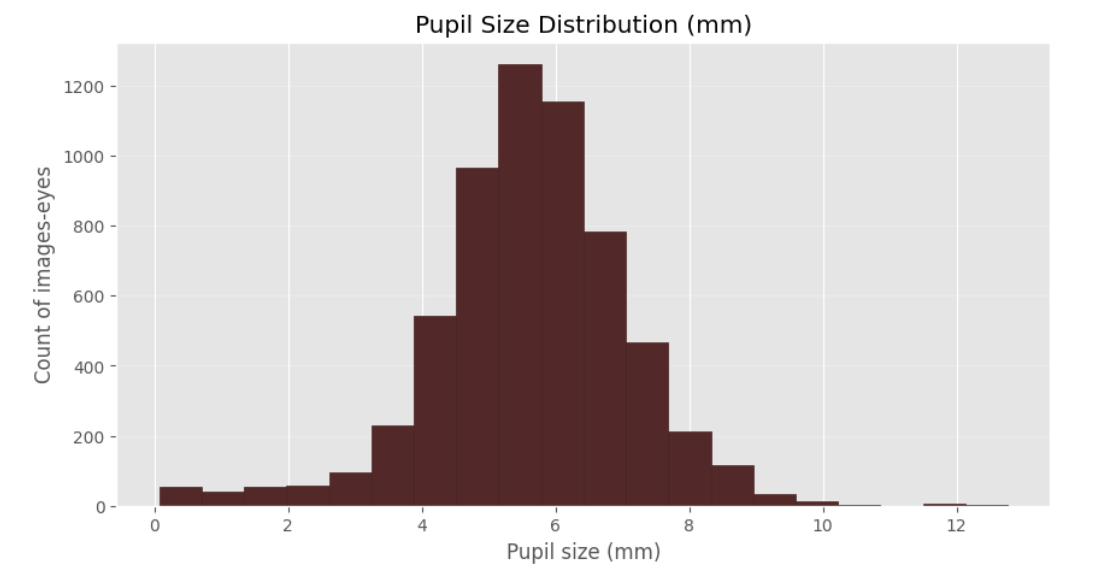
Using the same age split as in the retrospective analysis (<=15 vs >15), pediatric eyes showed consistently larger pupil diameters:
- <=15 years: n=1219 images-eyes, median 6.19 mm (IQR 5.53–6.98)
- 15 years and above: n=4865 images-eyes, median 5.50 mm (IQR 4.86–6.22)
- Median difference (pediatric − adult): +0.69 mm
The difference remains consistent across the distribution and is supported by the large number of eye images analysed.

Box-plot visualisation and median pupil size plot per year show a clear shift in the pediatric pupil-size distribution relative to adults.
This finding is consistent with established ophthalmic literature reporting larger pupil diameters in younger populations. [1] [2]
Why Larger Pupils Help VisionCheck
VisionCheck relies on pupil reflex geometry, where refractive information is encoded in patterns within the pupil region captured by the camera.
When pupil aperture is larger, the available optical signal within the pupil typically becomes stronger under the same capture conditions. From a screening perspective, this increases the likelihood that the recorded image contains sufficient signal for reliable VisionCheck inference.
Across the datasets analysed in this study, three observations point in the same direction:
- The Aarhus pediatric feasibility cohort showed strong practical performance.
- Segmentation-based analysis shows larger pupil diameters in children than adults.
Taken together, these observations provide a coherent technical explanation for the strong pediatric screening signal observed with VisionCheck.
Discussion
The combined evidence from this work indicates a consistent pediatric performance signal for VisionCheck.
The clinical feasibility study conducted in collaboration with Aarhus Ophthalmology Center demonstrates that children can successfully complete the VisionCheck capture workflow in a real clinical setting. Within this cohort, model predictions showed high accuracy and no obvious pediatric-specific degradation in performance.
The retrospective ProApp analysis extends these observations to a larger real-world dataset with age metadata. Pediatric captures maintained strong classification accuracy once quality constraints were satisfied.
The pupil-size analysis provides a physiological context that may help explain this pattern. Pediatric eyes in our dataset show larger pupil diameters compared to adults. Larger pupil apertures increase the amount of usable optical signal captured by the system, improving the probability of obtaining interpretable screening outputs.
Taken together, the evidence from the clinical cohort, the retrospective dataset, and the pupil-size analysis forms a coherent technical narrative: pediatric users show larger pupil apertures, larger pupils increase refractive crescent visibility, and this increased signal visibility aligns with the strong accuracy observed in pediatric VisionCheck captures.
From a deployment perspective, these findings suggest that VisionCheck may be well suited for pediatric refractive screening workflows. As a software-first system operating on standard smartphone hardware, it offers an objective and scalable approach that can complement traditional screening tools, particularly in environments where access to dedicated ophthalmic equipment is limited.
If your team is evaluating pediatric refractive screening workflows, you can book a short VisionCheck briefing with OptikosPrime to review clinical fit, deployment requirements, and pilot design options.
References
[^1] Guillon, Michel & Dumbleton, Kathryn & Theodoratos, Panagiotis & Gobbe, Marine & Wooley, C & Moody, Kurt. (2016). The Effects of Age, Refractive Status, and Luminance on Pupil Size. Optometry and vision science : official publication of the American Academy of Optometry. 93. 10.1097/OPX.0000000000000893. link
[^2] Lee YS, Kim HJ, Lim DK, Kim MH, Lee KJ. Age-specific influences of refractive error and illuminance on pupil diameter. Medicine (Baltimore). 2022 Jul 8;101(27):e29859. doi: 10.1097/MD.0000000000029859. PMID: 35801739; PMCID: PMC9259156. link
[^3] Aggarwal, Aditya; Gairola, Siddhartha; Upadhyay, Uddeshya; Vasishta, Akshay P.; Rao, Diwakar; Goyal, Aditya; Murali, Kaushik; Kwatra, Nipun; Jain, Mohit. (2022). Towards Automating Retinoscopy for Refractive Error Diagnosis. arXiv preprint arXiv:2208.05552. link
[^4] Bharadwaj, S. R.; Manzanera, S.; Artal, P. Eccentric Infrared Photorefraction: A Review of Evolution, Optical Design, Features and Applications. Journal of Bio-optics 2025, 1 (1), 4. Link
[^5] Van Eenwyk J, Agah A, Giangiacomo J, Cibis G. Artificial intelligence techniques for automatic screening of amblyogenic factors. Trans Am Ophthalmol Soc. 2008;106:64-73; discussion 73-4. PMID: 19277222; PMCID: PMC2646428. Link
